1. Introduction
Hip fractures are one of the most common and debilitating injuries presenting to emergency departments (EDs) worldwide, with an annual incidence of 1.26 million cases globally in 1990, projected to reach 4.5 million by 2050.1 These fractures predominantly affect the geriatric population, with 70% of patients experiencing severe pain (pain scores ≥7 out of 10).2 The management of acute hip fracture pain in the ED setting presents unique challenges, particularly given the vulnerability of the affected population to analgesic-related adverse effects.
Traditionally, systemic opioids have served as the cornerstone of acute pain management for hip fractures in emergency settings.3 However, this approach carries substantial limitations. Opioid administration in elderly patients is associated with high rates of adverse effects including sedation, respiratory depression, nausea, constipation, urinary retention, and delirium—complications that may substantially impact patient outcomes and prolong hospitalization.4,5 Moreover, approximately 40% of hip fracture patients in overcrowded EDs receive inadequate analgesia despite opioid administration.6
Regional anesthesia techniques, particularly the femoral nerve block (FNB), have emerged as promising alternatives to systemic analgesia. FNBs target the femoral nerve, which provides sensory innervation to the anterior thigh and hip capsule, making its blockade an ideal target for hip fracture analgesia.7 The advantages of FNB are compelling: targeted pain relief at the injury site, reduced systemic opioid exposure, preservation of cognitive function, and potentially improved patient outcomes.8,9
Integration of ultrasound guidance has revolutionized the performance of FNB, making it safer, more reliable, and increasingly accessible to emergency physicians.10,11 In the last 5 years, major medical organizations including the American College of Emergency Physicians, American Academy of Orthopedic Surgeons, and American College of Surgeons have endorsed ultrasound-guided nerve blocks as a standard of care in ED pain management.12–14 Now, emergency physicians are increasingly trained in UGNB procedures over landmark-based or nerve stimulator techniques.15
Despite growing adoption of ultrasound-guided femoral nerve blocks (UGFNBs), critical knowledge gaps persist. First, while numerous studies have evaluated FNB efficacy, the quality of evidence varies considerably, with many being observational or quasi-experimental designs.16–18 Second, previous systematic reviews have included heterogeneous patient populations across different clinical settings (ED, operating room, ward) and have combined studies using different techniques (ultrasound, nerve stimulator, landmark), limiting the applicability of findings to emergency practice specifically.19–21 Third, special populations such as patients with cognitive impairment or dementia—who constitute 30-45% of hip fracture patients and may benefit most from opioid-sparing analgesia—have been systematically excluded from most trials.22–24
This systematic review addresses these gaps by being the first synthesis to (1) isolate outcomes, efficacy, and safety of ultrasound-guided FNBs performed exclusively within ED settings, (b) focus solely on RCTs to provide the highest degree of evidence, and (3) include outcomes for patients with cognitive impairments, providing emergency physicians with specific, actionable evidence for current practice standards.
2. Methods
2.1. Eligibility Criteria
We performed a comprehensive search of peer-reviewed literature comparing UGFNB with standard care in ED patients with hip fractures. Studies were included if they: (1) were randomized controlled trials; (2) enrolled adult patients (≥18 years) with acute hip fracture; (3) performed UGFNB in the emergency department; (4) compared UGFNB to standard care (systemic analgesia); and (5) reported pain outcomes and/or opioid consumption. Only RCTs published from January 1, 1990 through January 15, 2026 were considered. Articles were restricted to the English language.
2.2. Information Sources and Search Strategy
A comprehensive literature search was conducted across four electronic databases: PubMed/MEDLINE, Embase, Scopus, and Google Scholar. Only the top 100 results from Google Scholar were included. The search strategy employed Medical Subject Headings (MeSH) terms and keywords related to femoral nerve blocks, hip fractures, emergency department, and ultrasound guidance.
2.3. Study Selection and Data Extraction
This systematic review was conducted following PRISMA guidelines. Initial search results were downloaded and exported to Covidence, and duplicates were automatically removed. One independent reviewer screened titles and abstracts using pre-defined eligibility criteria. Articles marked for inclusion proceeded to full-text review.
From each included study, we extracted: study design characteristics, sample size, patient demographics, ultrasound technique details, local anesthetic type and volume, pain assessment methods, adverse events, and follow-up duration. Primary outcomes included: pain scores, opioid consumption, and proportion of patients achieving meaningful pain relief. Secondary outcomes included time to pain relief, adverse events, length of stay, and outcomes in special populations.
2.4. Synthesis Methods
Due to heterogeneity in study designs, outcome measures, timing, and comparators, narrative synthesis was performed. Pain scores were converted to a 0-10 scale and opioid doses to oral morphine milligram equivalents (MME) using standard conversion factors.
3. Results
3.1. Study Selection
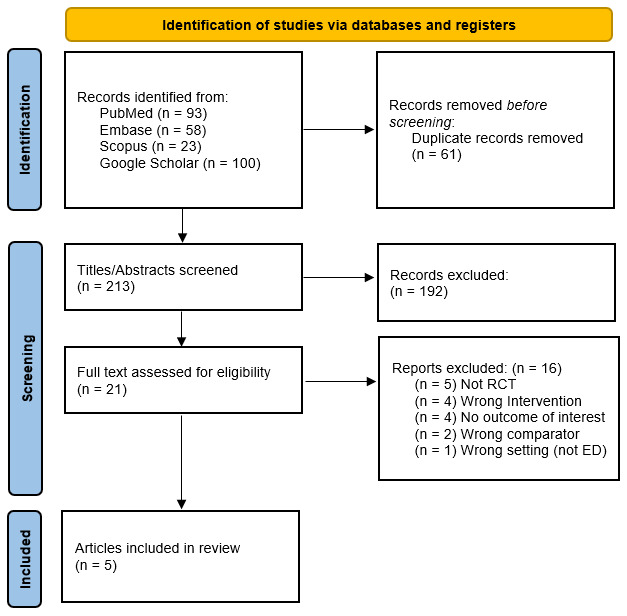
Our initial database search identified 274 records, reducing to 213 unique citations after duplicate removal. After screening the titles and abstracts, 20 studies were selected for full-text review, of which five RCTs met all inclusion criteria (Figure 1). Studies were conducted in Turkey,24 France,25 Iran,26 United Kingdom,27 and Sweden.28 All studies utilized high-frequency linear ultrasound transducers (7-12 MHz) for nerve visualization and in-plane needle insertion technique. The trials collectively enrolled 551 patients, with sample sizes ranging from 30 to 266 patients (Table 1).

3.2. Pain Outcomes
All five RCTs demonstrated significant pain reduction with UGFNB compared to standard care. Altunbaş et al. (2026)24 demonstrated the most rigorous double-blind design, finding UGFNB patients experienced median pain score reduction of 4 points versus 2 points with intravenous (IV) fentanyl at 20 minutes (median difference 2 points, 95% CI 1-2, p<0.001). Mayel et al. (2022)25 found similar pain reductions in both groups at 15 minutes, but UGFNB achieved comparable analgesia without opioid-related side effects.
For sustained pain relief, Unneby et al. (2017)26 provided the most comprehensive temporal analysis in 266 patients, demonstrating that UGFNB significantly reduced self-rated VAS pain scores from baseline to 12 hours post-admission (p<0.001), with significant reductions at 2 hours (p=0.004, effect size r=0.37) and 12 hours (p=0.001, effect size r=0.44). Rowlands et al. (2018)27 found cumulative pain at rest was significantly lower in the UGFNB group (median 2 vs 5, p=0.043), though dynamic pain scores showed no difference.
Gerlier et al. (2024)28 found median time to pain relief (pain score ≤3) was 1.0 hour in the UGFNB group compared to 2.0 hours in standard care, with a median difference of 1.0 hour (95% CI 0.0-3.0), though this did not reach statistical significance. Within 6 hours, 93% (14/15) of UGFNB patients versus 87% (13/15) of standard care patients achieved meaningful pain relief.
3.3. Opioid Consumption
All five studies consistently demonstrated 56-80% reductions in opioid consumption with UGFNB. Altunbaş et al. (2026)24 reported only 21.1% of UGFNB patients required rescue analgesia within four hours compared to 61.5% in the fentanyl group (p<0.001), representing a 66% relative reduction. Gerlier et al. (2024)28 demonstrated 60% reduction in preoperative opioid consumption over 48 hours: median 6 MME versus 15 MME (p<0.001). Unneby et al. (2017) found UGFNB patients required 60% less intravenous opioids in the orthopedic ward (mean 2.3±4.0 mg vs 5.7±5.2 mg, p<0.001), with significantly lower proportions requiring any opioid administration: 39.4% versus 83.4%.
3.4. Adverse Events
A striking finding was the favorable safety profile of UGFNB. Across all 551 patients, zero serious UGFNB-related complications were reported—no cases of permanent nerve injury, local anesthetic systemic toxicity, major hematoma, infection, or vascular injury requiring intervention. Altunbaş et al. (2026)24 reported zero FNB complications, while the IV fentanyl group experienced nausea (23%), dizziness (15%), headache (9.6%), and hypotension (5.7%). Gerlier et al. (2024)28 documented opioid adverse events in 93.3% of standard care patients versus 53.3% of UGFNB patients. Unneby et al. (2017) found no adverse events among 129 UGFNB patients despite 36 different anesthesiologists with varying experience performing blocks.
3.5. Special Populations: Cognitive Impairment
Two studies specifically addressed outcomes in patients with cognitive impairment, representing a major advancement for this vulnerable population. Altunbaş et al. (2026)24 included 43 cognitively impaired patients (41.3% of total), using validated pain assessment tools (PAINAD for impaired patients, NPRS for intact patients). In cognitively impaired patients, median PAINAD score reduction was 4 points with UGFNB versus 2 points with IV fentanyl (p<0.05).
Unneby et al. (2017)26 included 120 patients (45.1%) with dementia diagnoses. Among dementia patients, proxy VAS assessments showed significant pain score decreases in the UGFNB group at 6 hours (p=0.007, effect size r=0.425), while no significant change occurred in controls. Dementia patients receiving UGFNB required 64% less IV morphine (mean 2.1±3.3 mg vs 5.8±5.0 mg, p<0.001), with significantly lower proportions requiring opioids: 41.7% versus 83.3% (p<0.001).
3.6. Procedural Characteristics and Feasibility
Mean procedure times ranged from 7 to 14 minutes, compatible with busy ED workflows. Crucially, UGFNB can be successfully performed by emergency physicians after brief training. In Gerlier et al.,28 seven emergency physicians performed UGFNBs after standardized training involving 2 hours theory, 1 hour ultrasound practice, and 2 supervised procedures; five physicians were novices with no prior UGFNB experience. Unneby et al. achieved consistent efficacy and zero complications despite 36 different anesthesiologists with varying experience performing blocks. Altunbaş et al. achieved 100% procedural success with three researchers having at least 2 years of practical experience administering UGFNBs.
All studies used standard ED ultrasound equipment with high-frequency linear transducers (7-12 MHz) and similar anatomic approaches: patient supine with slight hip abduction, transducer at inguinal crease, femoral nerve identified lateral to femoral artery, in-plane needle insertion with visualization of local anesthetic spread.
3.7. Secondary Outcomes
Two studies reported no significant differences in ED or hospital length of stay between groups.27,28 Rowlands et al. found no difference in time to surgery (mean 15.5±10.3 hours vs 16.2±10.1 hours, p=0.565) or functional outcomes assessed by Cumulated Ambulation Score (median 6 vs 7, p=0.76), confirming UGFNB does not delay surgical intervention or impair early mobilization.
Gerlier et al.28 noted a trend toward reduced delirium with UGFNB (0% vs 7.4%, p=0.118) though not statistically significant. The authors also tracked bowel movements using Bristol Stool Charts for three postoperative days, defining constipation as no bowel movements on any of the three days. Constipation occurred in 56% (30/54) of controls vs. 50% (25/50) of UGFNB patients (p=0.57), showing no significant difference.
4. Discussion
This systematic review of five RCTs provides robust evidence that ultrasound-guided femoral nerve blocks offer superior pain control and substantially reduced opioid consumption compared to standard care in ED patients with hip fractures, with a favorable safety profile. The consistency of findings across diverse geographic settings, populations, and methodologic approaches strengthens confidence in these conclusions and supports the integration of UGFNB into routine emergency practice.
The 56-80% reduction in opioid consumption represents a clinically meaningful benefit with potential to substantially decrease opioid-related adverse events.
The complete absence of serious UGFNB-related complications across 551 patients and multiple practice settings is noteworthy. This safety profile represents a substantial improvement over historical landmark-based or nerve stimulator techniques, and agrees with findings from previous studies that directly compare these techniques with ultrasound methods.29,30 This improvement can be explained by ultrasound guidance enabling direct visualization of vascular structures, real-time needle tip assessment, and confirmation of extravascular anesthetic spread. The contrast between near-zero UGFNB complications and substantial opioid-related adverse events (nausea 21-23%, dizziness 15%, altered mental status up to 28.6% in controls) strongly favors UGFNB.
Our findings align with but extend beyond previous systematic reviews. The 2020 Cochrane review by Guay et al. included 49 studies across all settings and techniques but only a small subset used ultrasound guidance in ED settings.8 Similarly, Ritcey et al.'s 2016 systematic review of ED-based regional blocks for hip fractures included both RCTs and observational studies using various techniques.20 Our exclusive focus on ultrasound-guided ED-based RCTs provides higher-quality evidence specific to current standards. Importantly, previous reviews do not include trials with cognitively impaired patients. Our review demonstrates this limitation has been addressed, with two studies24,26 providing robust evidence for UGFNB efficacy in 120 patients with dementia—a critical advancement given this population’s heightened vulnerability to opioid-related harm.
4.1. Strengths & Limitations
This is the first systematic review of UGFNBs administered exclusively in the ED setting. The strengths of this review lie in its rigor in searching the literature and the novel inclusion of trials with dementia patients, which addresses a critical evidence gap. Despite only five studies being included, the comprehensive search strategy is likely to have identified all of the available RCTs comparing UGFNBs with standard analgesia in the ED to date. By excluding non-ultrasound techniques, we provide compelling and unique evidence directly applicable to contemporary practice in emergency settings.
Limitations include heterogeneity in local anesthetic choice, dosing, timing, and outcome measures, limiting potential for meta-analysis. All studies were conducted at academic centers in developed countries; generalizability to community EDs or resource-limited settings requires future validation. Two studies had relatively small samples (15-20 per group), limiting power for detecting rare complications or significant differences in secondary outcomes. Most studies focused on acute ED pain relief; longer-term outcomes including postoperative pain trajectories and rehabilitation progress remain underexplored.
4.2. Clinical Implications
These findings support integrating UGFNB into routine ED management of hip fractures. Evidence demonstrates feasibility for emergency physicians at all levels. Standardized training programs of 3-8 hours enable safe, effective UGFNB performance, with novice operators achieving success rates comparable to experienced practitioners after brief training. Standard ED ultrasound machines with high-frequency linear transducers are sufficient; no specialized equipment is required.
UGFNB should ideally be performed immediately upon radiographic confirmation and before ward transfer. Physicians should consider UGFNB even in patients who received initial opioids. Patients with cognitive impairment, dementia, or delirium remain ideal candidates and may be preferential given heightened opioid sensitivity. Routine contraindications (local anesthetic allergies, patient refusal, injection site infection) should still be considered.
Future studies should include more cognitively impaired patients and report outcomes such as postoperative delirium incidence and functional recovery. Standardized protocols for UGFNB administration regarding dose and timing would benefit the field.
5. Conclusions
The evidence supports UGFNB as a safe, effective, and practical pain management strategy that should be considered standard practice for hip fracture patients presenting to the ED. UGFNB delivers clinically meaningful pain score reductions sustained over 12+ hours and dramatic decreases in opioid consumption (56-80%). Zero serious complications across 551 patients and maintained benefits in vulnerable populations suggest broad safety and applicability. The technique can be safely performed by emergency physicians after brief training, with success rates comparable to experienced anesthesiologists. Future research should focus on RCTs including elderly or dementia patients and reporting longer-term quality of life outcomes.