

Introduction
Enhanced Recovery After Surgery (ERAS) is a multidisciplinary, protocol-driven approach to the perioperative management of surgical patients. Introduced approximately two decades ago, ERAS has transformed surgical practice by reducing postoperative complications and shortening hospital length of stay.1,2 The primary objective is to optimize surgical outcomes while enhancing the patient experience and accelerating recovery.3
ERAS protocols require collaboration among anesthesiologists, surgeons, nurses, and designated ERAS coordinators, often physician assistants or advanced practice nurses.4 Each discipline plays a defined role: anesthesiologists focus on prehabilitation, anesthetic planning, and perioperative optimization; surgeons employ minimally invasive techniques; and coordinators ensure consistent application of standardized practices. Collectively, these measures enable individualized care with an emphasis on early mobilization, nutritional support, and proactive complication prevention.5,6
Beyond clinical outcomes, ERAS pathways have been shown to reduce healthcare costs by anticipating and mitigating postoperative complications.7 For example, hospitals adopting ERAS protocols have demonstrated reductions in mean hospital stay by over 20%8 and total surgical costs by approximately 21%.9 These efficiencies are achieved through targeted strategies: optimizing nutritional status, minimizing opioid use in favor of non-opioid analgesics such as NSAIDs,10 reducing drains and catheters early, and ensuring early resumption of oral intake and mobility.
Given the success of ERAS programs, these protocols are now implemented in more than 20 countries.11 However, adoption varies across healthcare systems, influenced by resource availability, cultural practices, and institutional priorities. Bibliometric analyses provide valuable insight into how ERAS principles are disseminated worldwide, highlighting trends in publication output, international collaboration, and institutional leadership. The present study aims to map the global research landscape surrounding ERAS protocols, identifying influential contributors and assessing patterns of dissemination.
Methods
Study Design
Bibliometric analysis is a quantitative methodology used to evaluate and visualize patterns within the scientific literature. It enables researchers to identify trends in publication activity, authorship, and collaboration, while also highlighting gaps that may inform future investigation.12,13
Data Source and Search Strategy
Data for this study were obtained from the Web of Science (WoS) Core Collection, a multidisciplinary database that provides extensive coverage of high-impact scientific literature. WoS was selected because of its rigorous indexing standards and its established use in bibliometric research across the biomedical sciences. The search was restricted to the topic field, encompassing article titles, abstracts, and keywords.
The search strategy included the terms: “enhanced recovery after surgery” OR “ERAS protocol.” Publications from 2002 through 2025 were retrieved. No exclusions were applied with respect to language, punctuation, capitalization, or document type, thereby ensuring maximal inclusivity of relevant literature. Both original articles and reviews were considered eligible.
Data Extraction and Analysis
Retrieved records were first analyzed using the WoS analytical tools to generate treemaps and descriptive statistics. Column charts were constructed in Microsoft Excel (version 16.101) using the raw WoS data. For advanced visualization of keywords, the dataset was exported as a tab-delimited text file containing complete bibliographic records. These files were then imported into VOSviewer software (version 1.6.2; Leiden University, Leiden, Netherlands).14 In this visualizations, each item is represented as a node (circle), with its size proportional to its contribution or frequency. Connections between nodes are represented by colored links, where thickness and length indicate the strength of association (total link strength).
Data elements extracted included: article title, abstract, author(s), keywords, publishing journal, document type, country of origin, and citation counts. These metrics enabled a comprehensive assessment of publication patterns, collaborative networks, and thematic foci within the ERAS literature.
Results
The search yielded a total of 18,681 documents, of which 2773 were review articles, and 8818 were open access articles.
Institutional Contributions
When the web of science was searched for institutions, Harvard Medical School and its affiliates had the highest number of publications at 1387, followed by Mayo Clinic (258 documents) and Johns Hopkins (244 documents). The most prolific institutions outside of the United States were McGill University in Canada (215 documents), Centre Hospitalier Universitaire Vaudois Chuv in Switzerland (191 documents) and Sichuan University in China (191 documents). [Figure 1]. When institutions with departmental affiliations were searched, Johns Hopkins (258 documents) had the highest number, followed by Stanford University (231 documents) [Figure 2].
_da.png)

Geographic Distribution
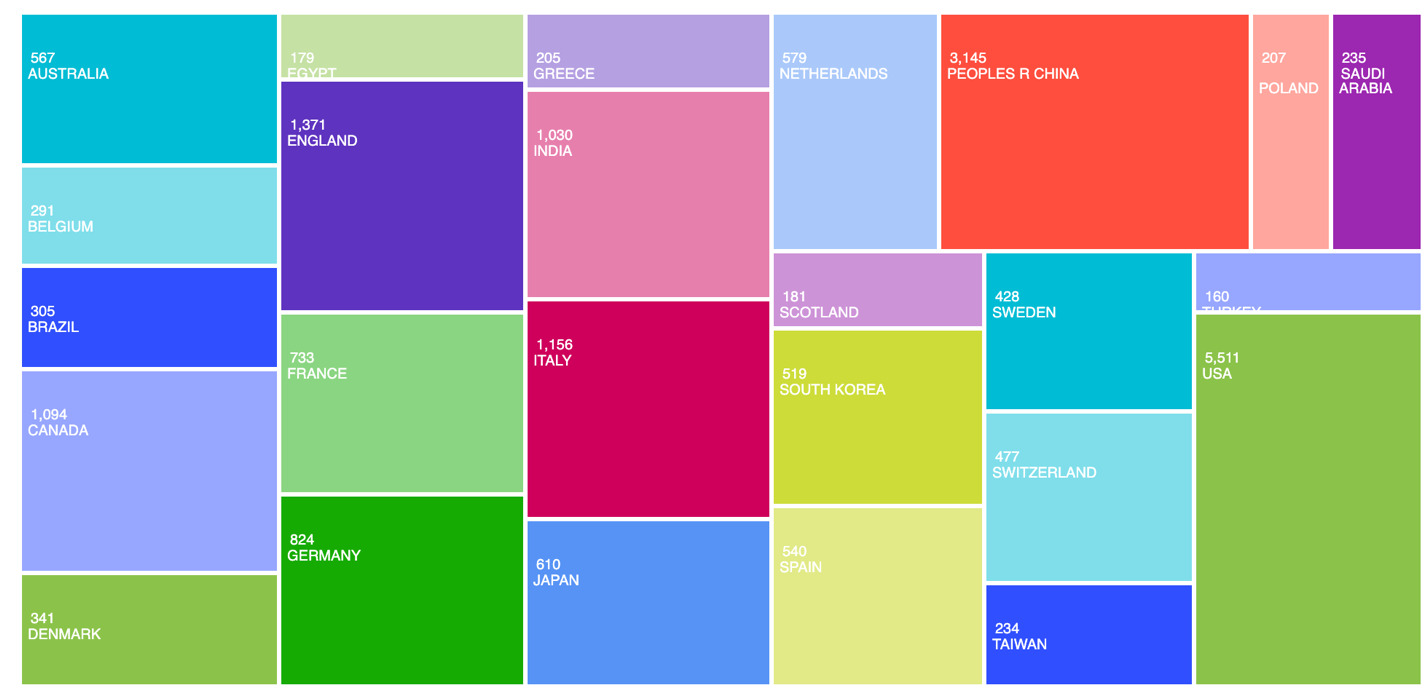
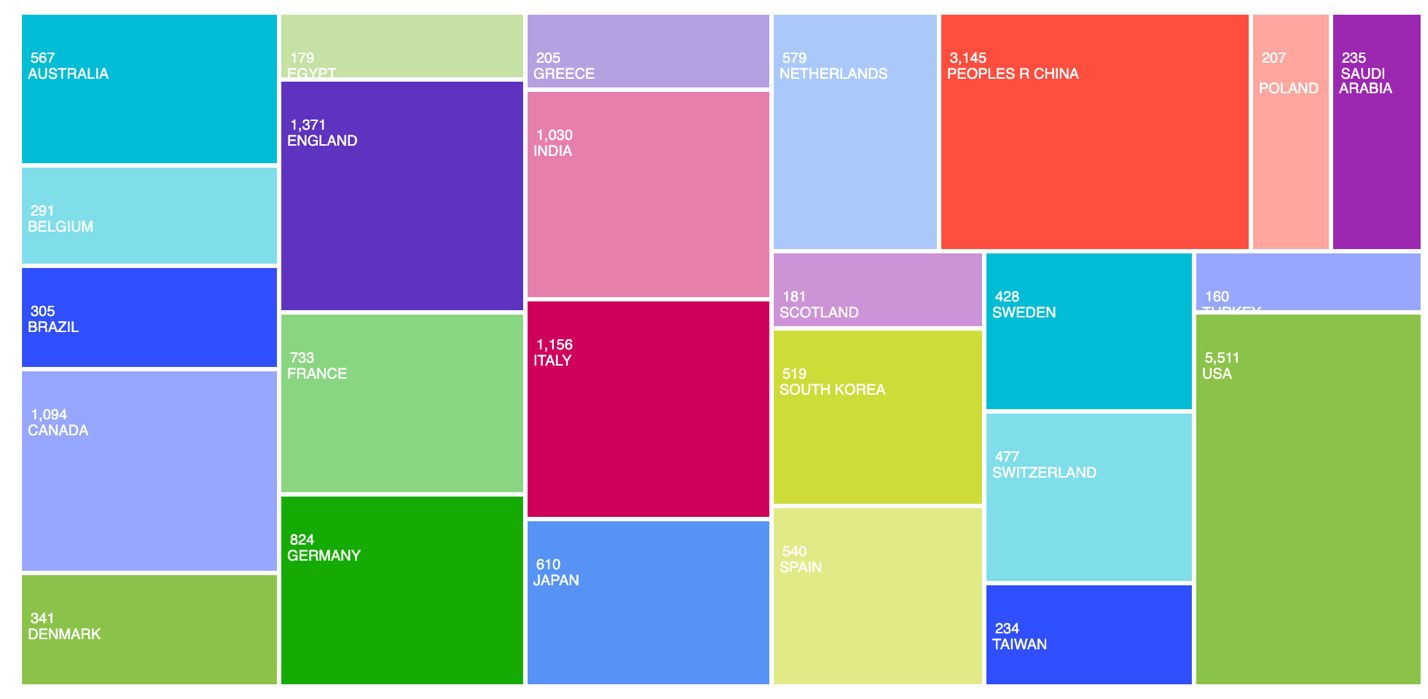
The top five most prolific countries were the United States (5511 documents), China (3145 documents), Italy (1156 documents), Canada (1094 documents), and India (1030 documents) [Figure 3].
Publication Trends
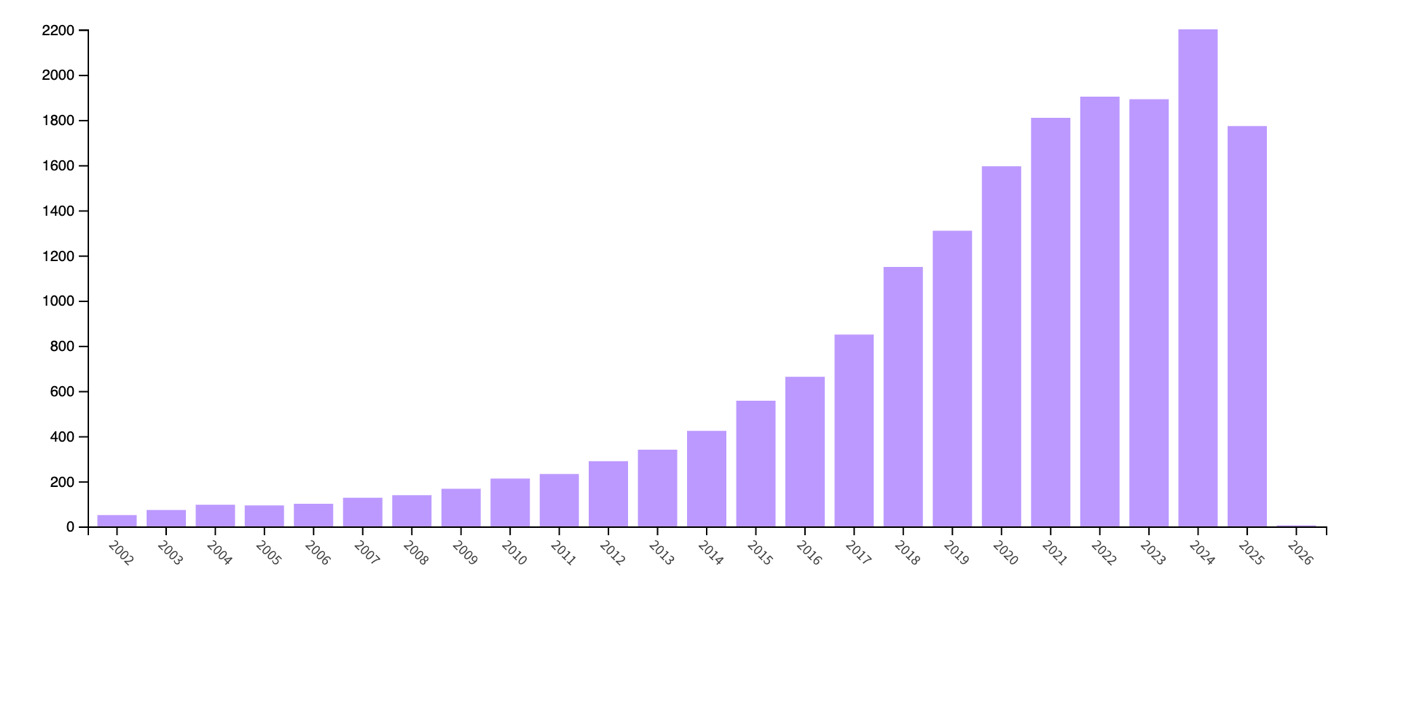
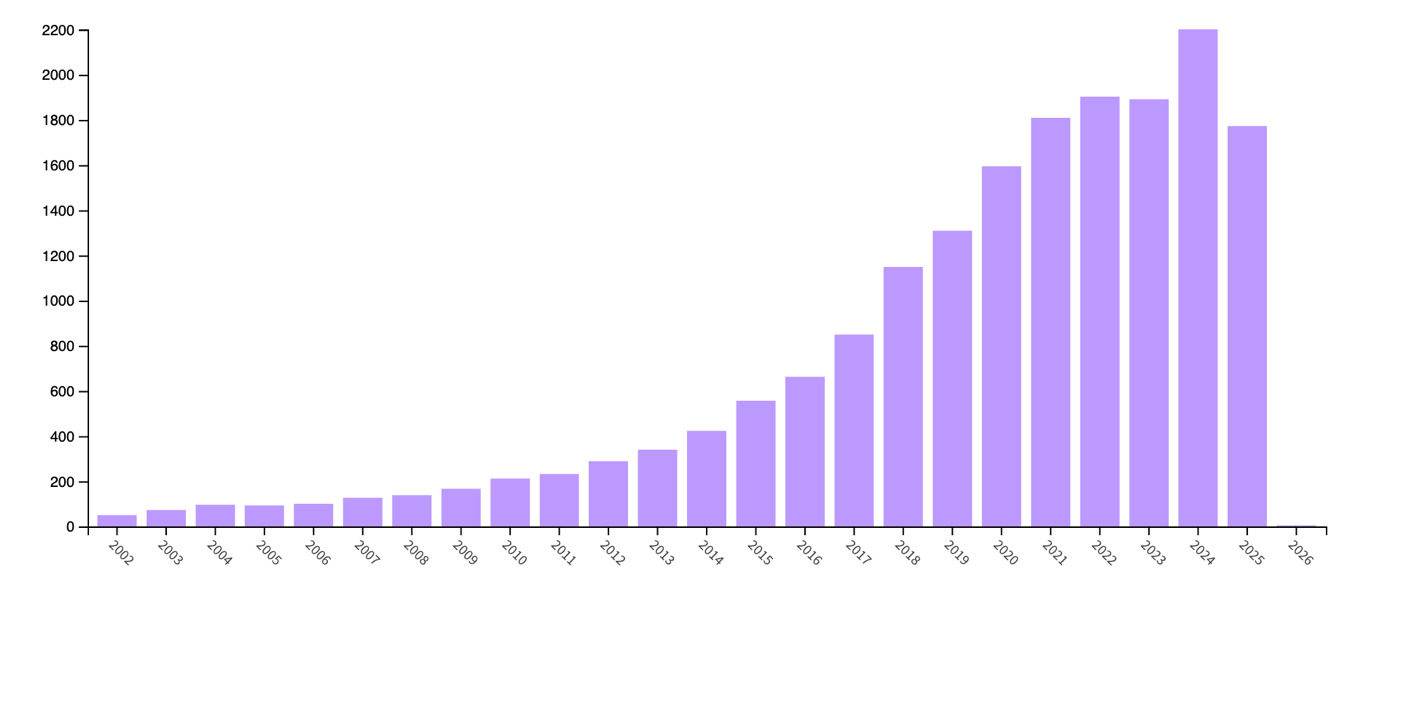
Between 2002 and 2025, the volume of ERAS-related publications steadily increased, reflecting the growing adoption and refinement of ERAS practices worldwide [Figure 4].
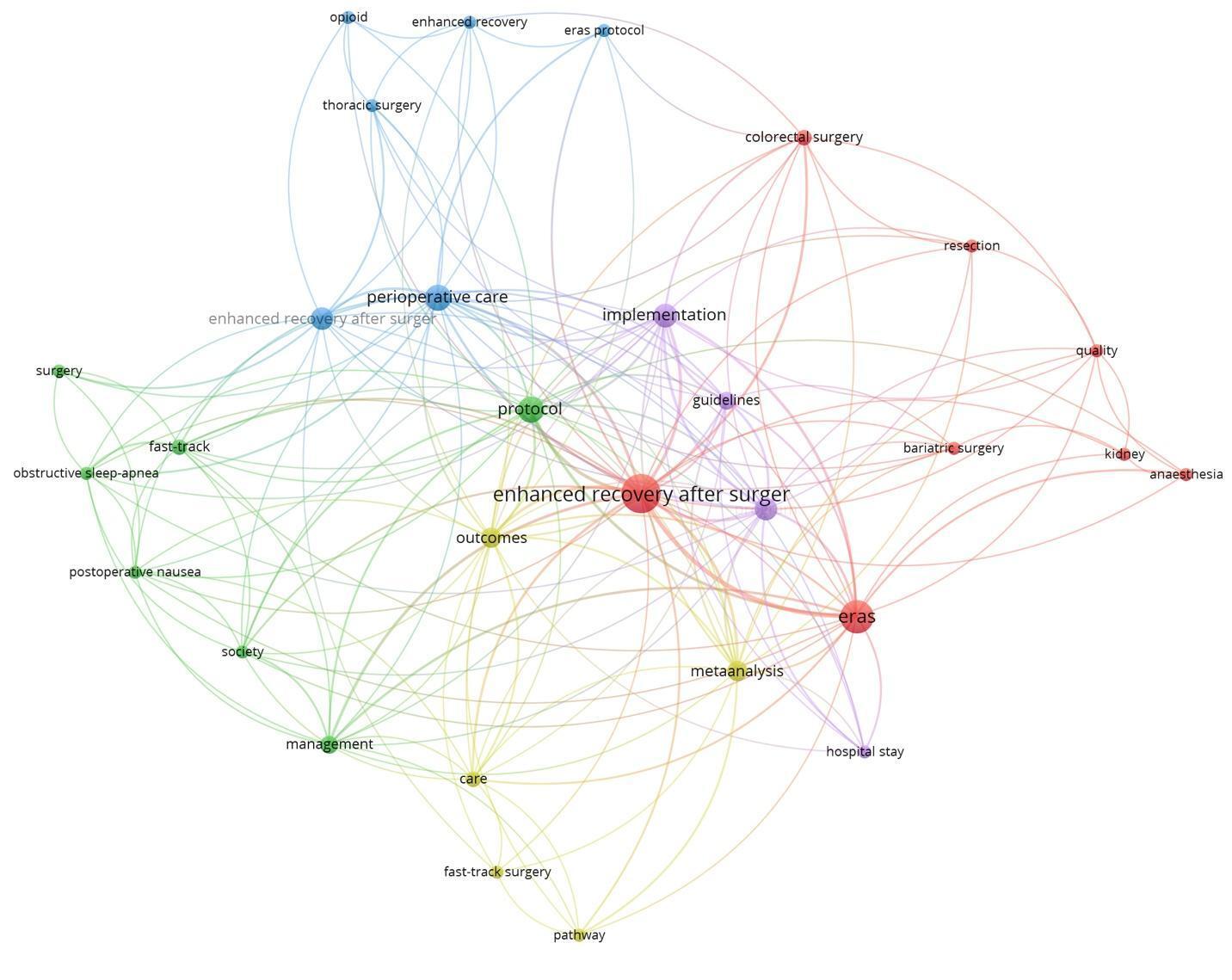
Thematic Analysis
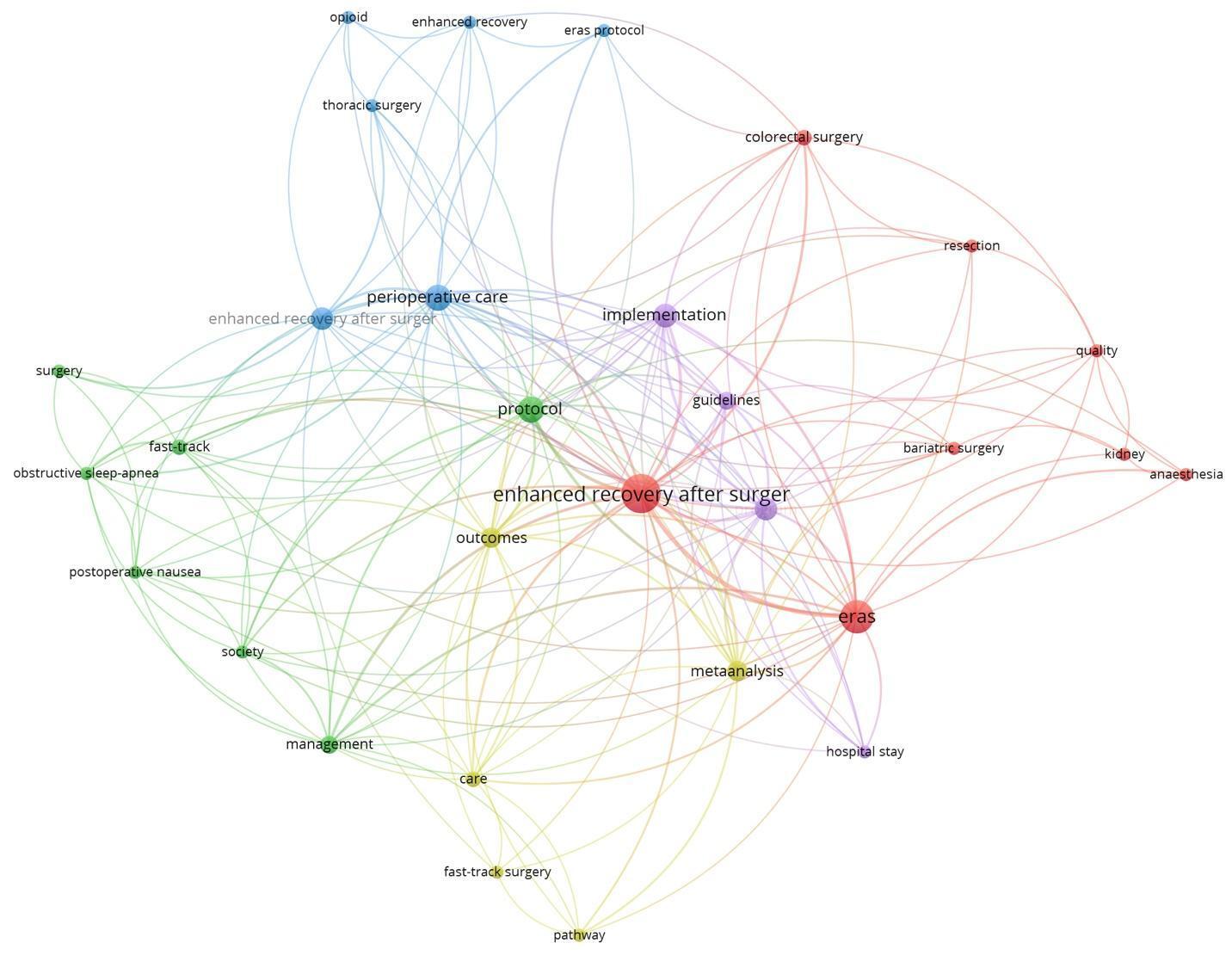
Keyword mapping reveals broad themes such as perioperative care, and complications nausea and obstructive sleep apnea as emerging themes. The three surgical fields noted are colorectal surgery, thoracic surgery and bariatric surgery [Figure 5].
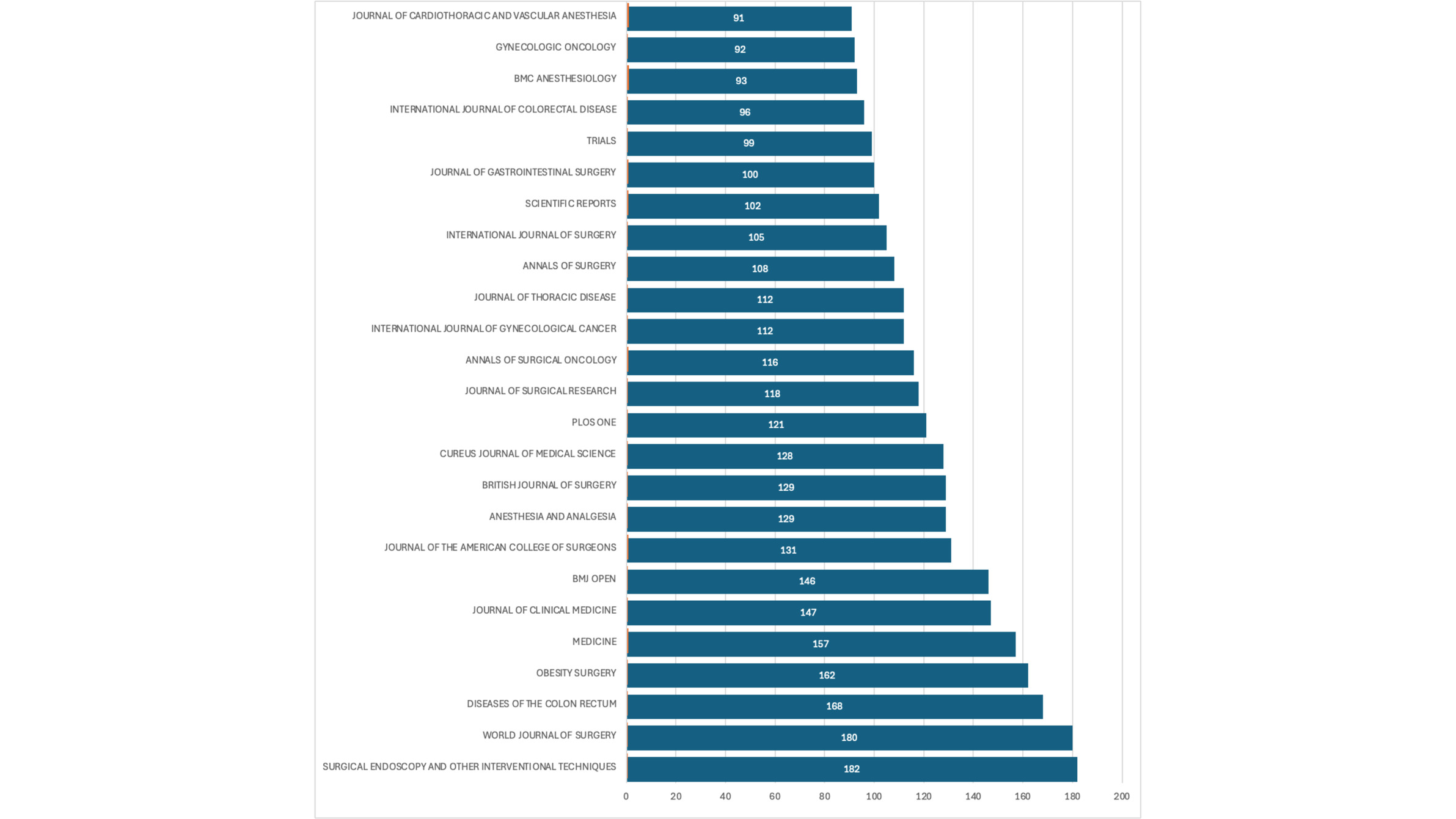
Journal Publication
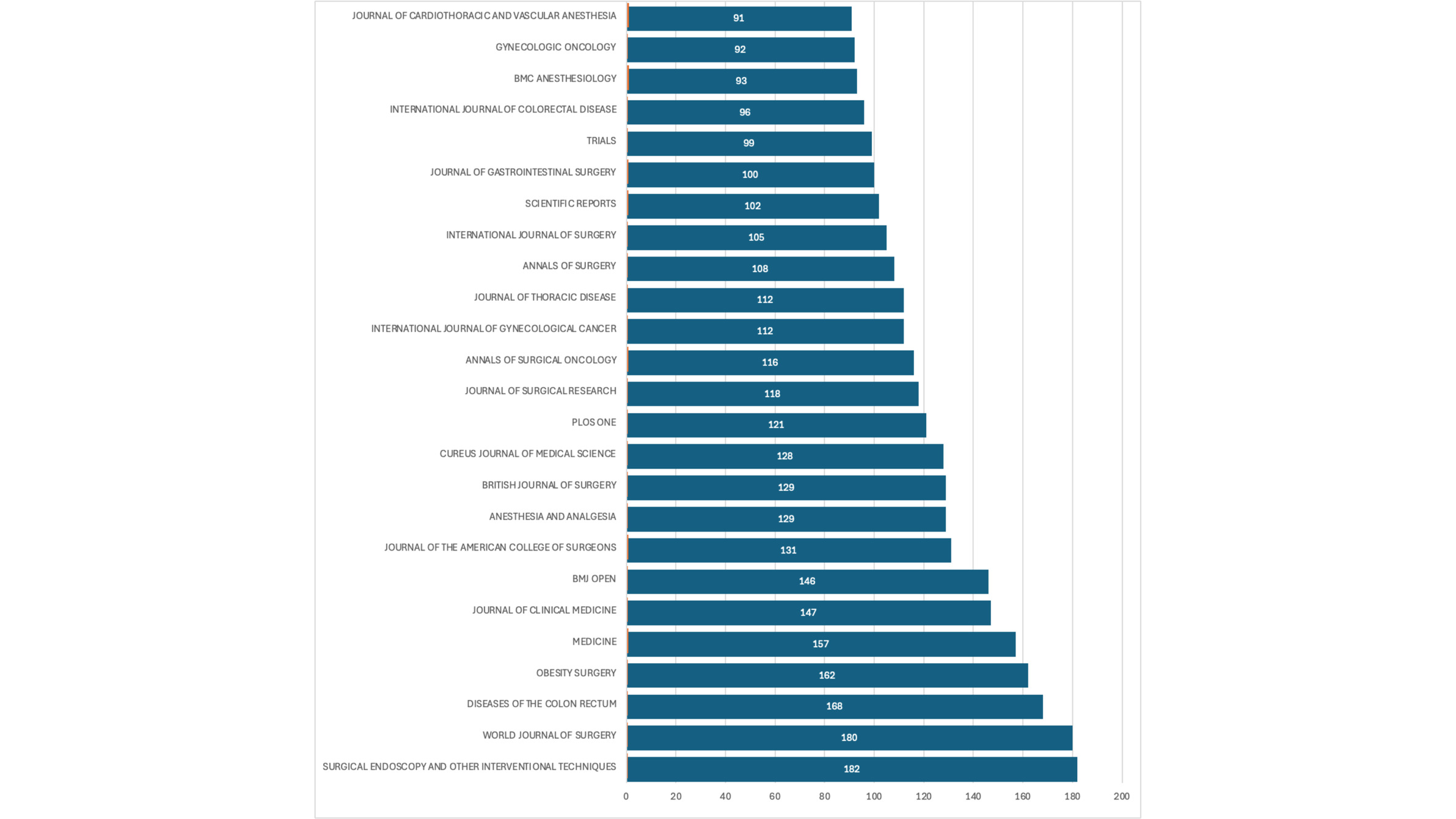
Figure 6 depicts the top 25 journals (in terms of numbers) where ERAS papers have been published. The top four journals were: Surgical Endoscopy and Other Interventional Techniques (182 documents), World Journal of Surgery (180 documents), Diseases of the Colon and Rectum (168 documents) and Obesity Surgery (162 documents).
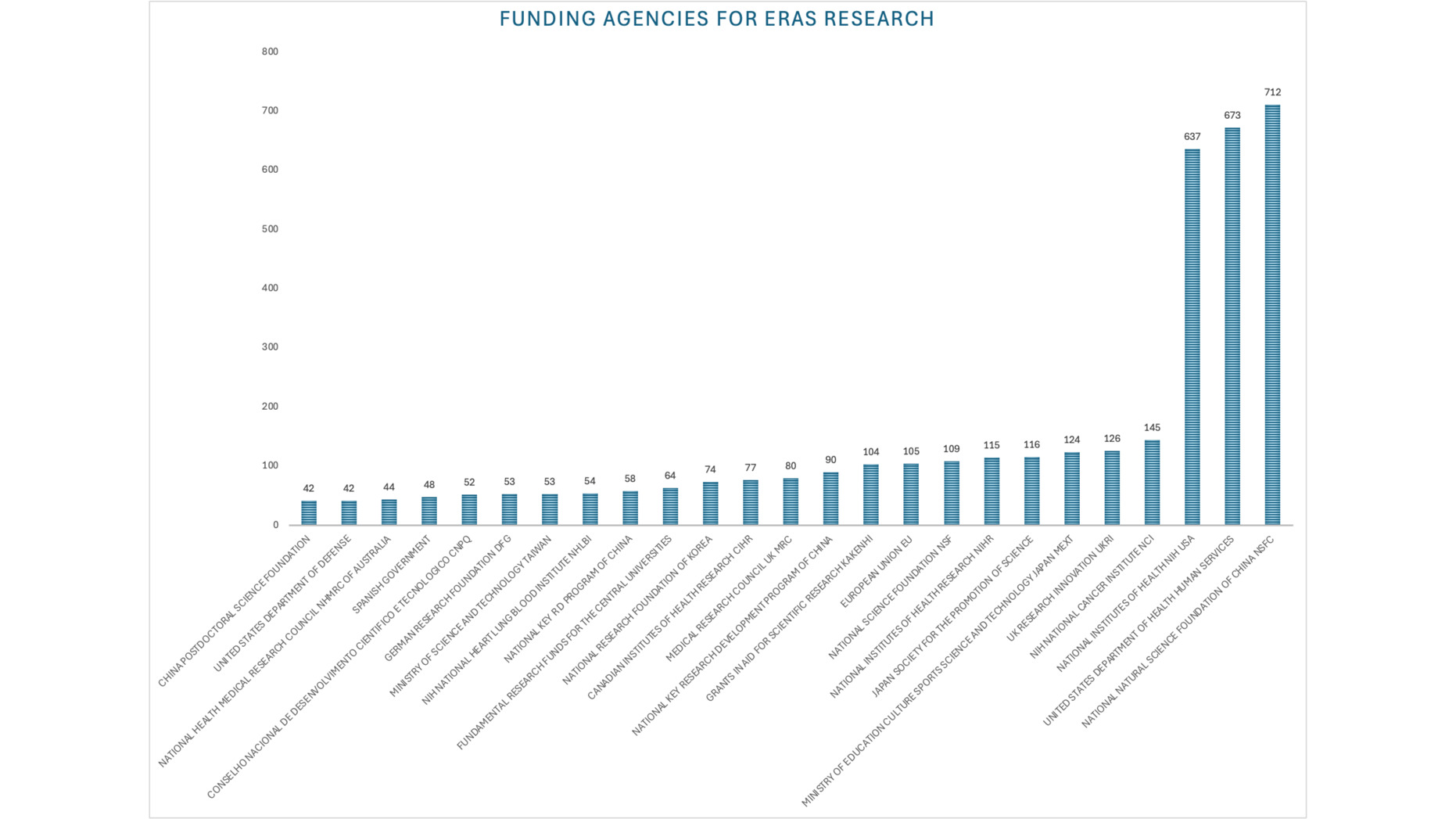
Funding Sources
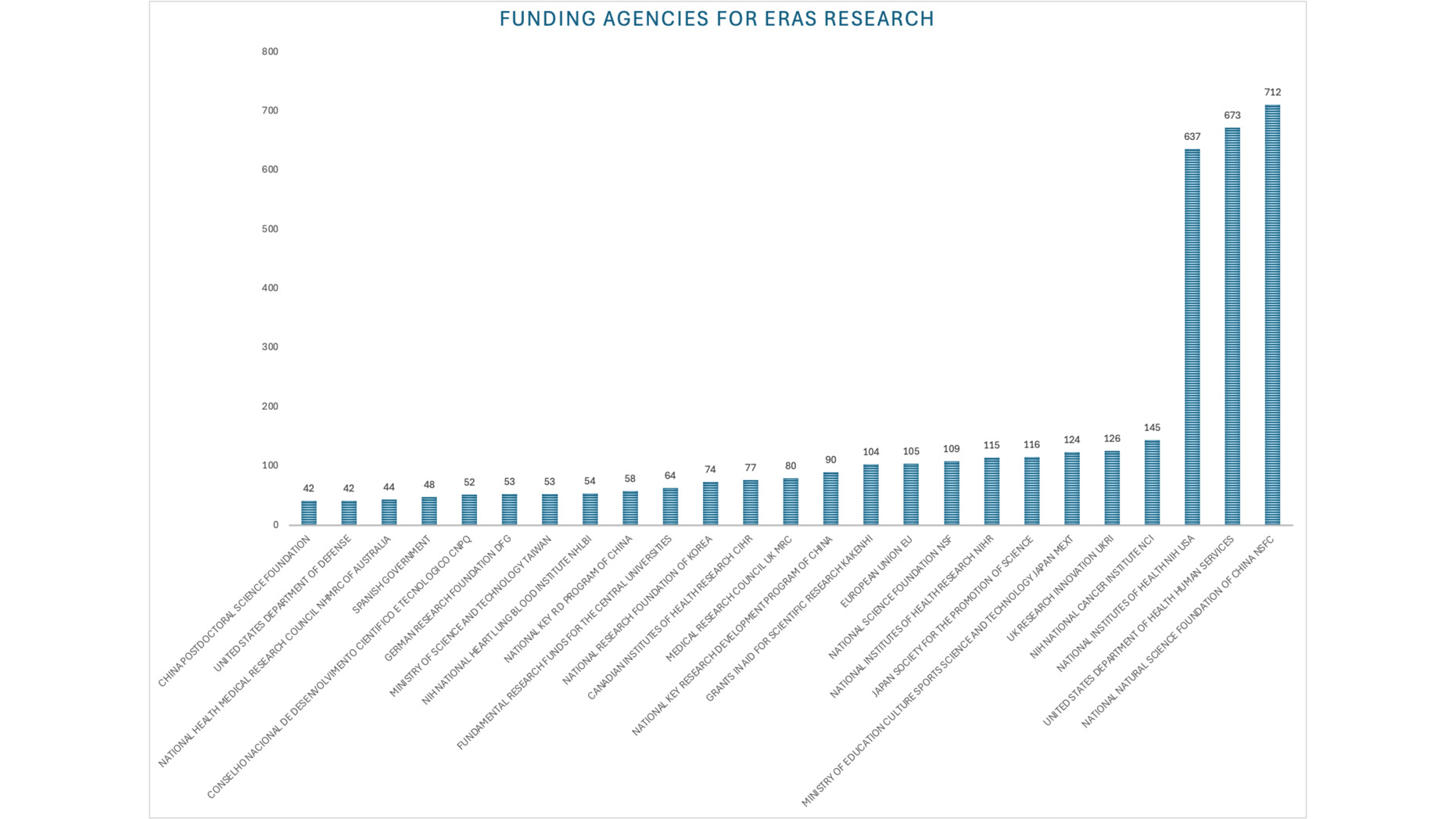
The countries that devoted the most research funding to ERAS were China via the National Natural Science Foundation of China, followed by the United States via the department of health and Human Services and the National Institutes of Health [Figure 7].
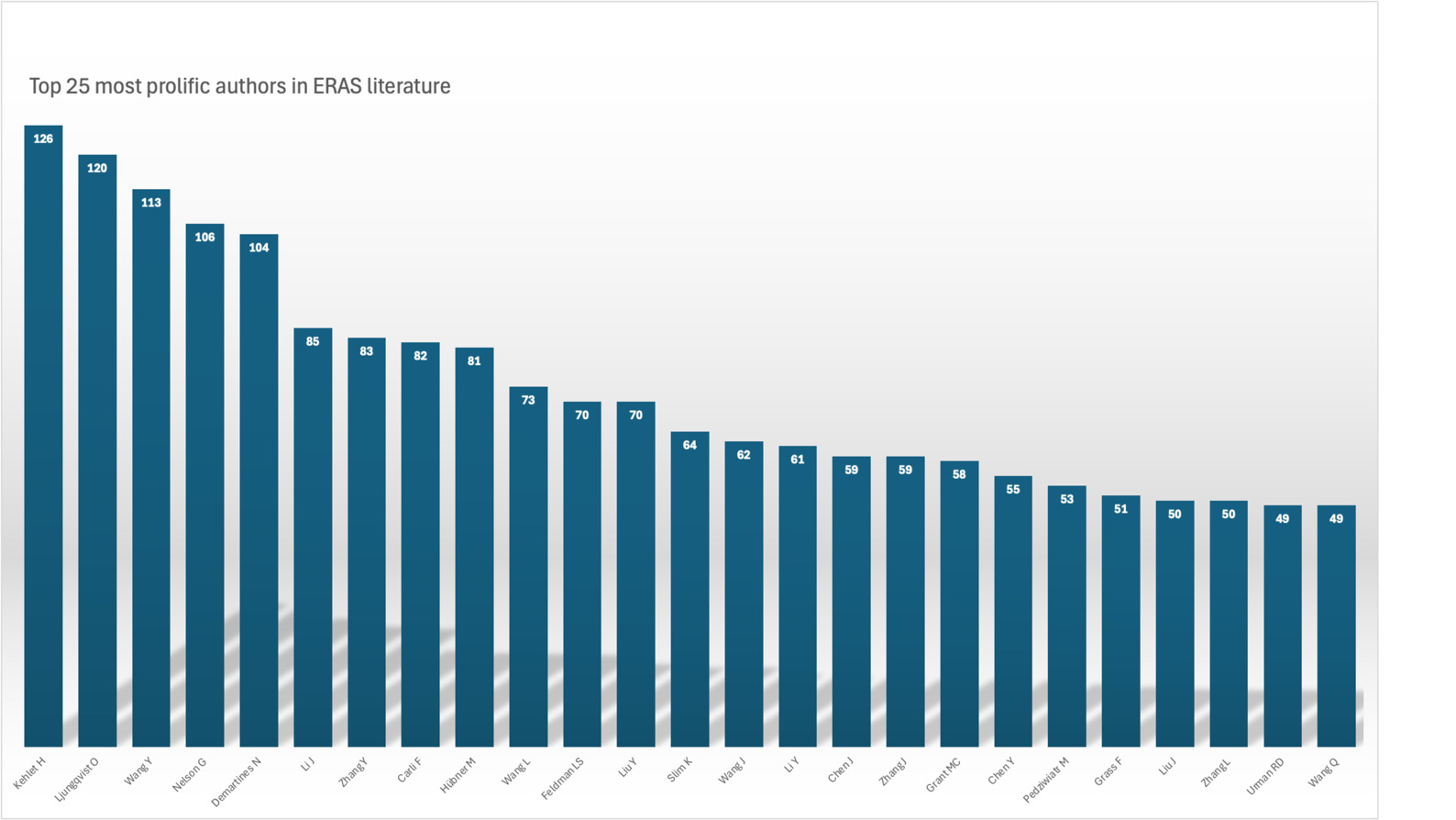
Prolific Authors
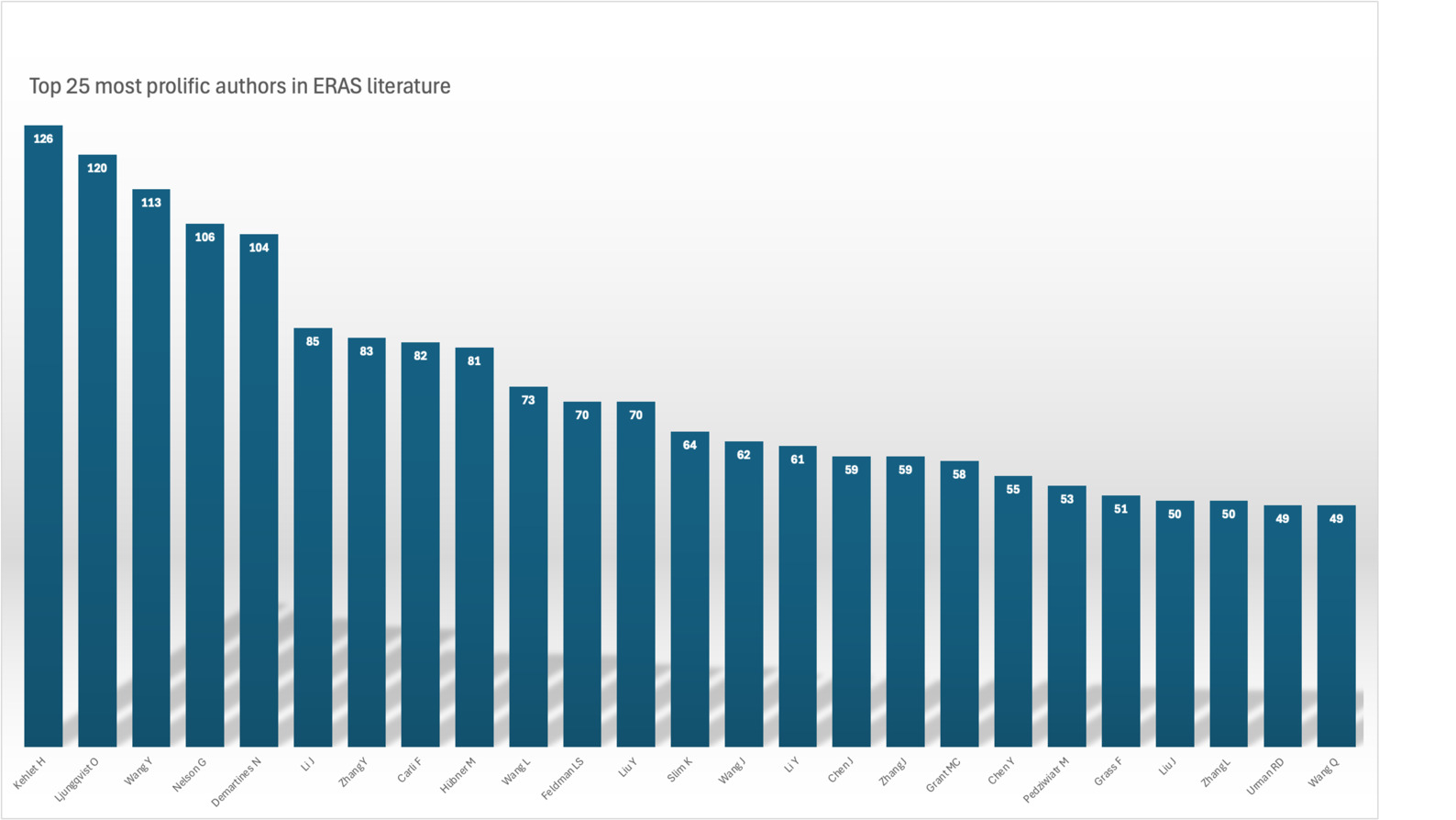
The top 25 most prolific authors in ERAS publications are listed in Figure 8. Henrik Kehlet, from the Section of Surgical Pathophysiology, Copenhagen University Hospital, Rigshospitalet, Denmark was the most prolific author followed by Olle Ljungqvist at the School of Medical Sciences, Department of Surgery, Örebro University, Örebro, Sweden [Figure 8].
Discussion
The implementation of ERAS protocols has consistently demonstrated reduced complication rates, shorter hospitalization, and enhanced recovery.15 The bibliometric analysis confirms a sustained growth in ERAS-related literature over the past two decades, coinciding with global dissemination of these practices. While the United States and China dominate publication output, adoption in developing countries remains limited due to resource constraints and healthcare access disparities.16,17
Institutional analysis revealed that academic centers such as Harvard Medical School have been instrumental in driving ERAS scholarship. Collaborative networks show clustering of countries by geography and historical ties, such as the United States with Canada, or the United Kingdom with India, Egypt, and Brazil.
Early adoption in the United Kingdom focused on colorectal surgery, where ERAS protocols—including minimally invasive surgery and preoperative carbohydrate loading—significantly reduced recovery time, accelerated return of bowel function, and improved cardiopulmonary outcomes. Similar benefits have been observed in South Korea, where colorectal ERAS implementation reduced complication rates,18 and in France, where adoption remains limited but patient education and early mobilization strategies have improved outcomes.19
Despite initial resistance to protocols that contradicted traditional perioperative practices, accumulating evidence has supported ERAS integration worldwide.20 The findings of this bibliometric analysis illustrate both the progress achieved and the barriers that remain in ensuring equitable global implementation.
Conclusion
This bibliometric analysis demonstrates the expanding influence of ERAS protocols in perioperative medicine. By mapping publication output, institutional contributions, and international collaborations, the study highlights the pivotal role of leading countries and institutions in advancing ERAS adoption. While challenges persist in resource-limited settings, the overall trajectory reflects increasing global acceptance. Ultimately, ERAS protocols exemplify a patient-centered, cost-effective, and evidence-based model of perioperative care, underscoring their value as a standard of practice in anesthesia and surgery.