Introduction
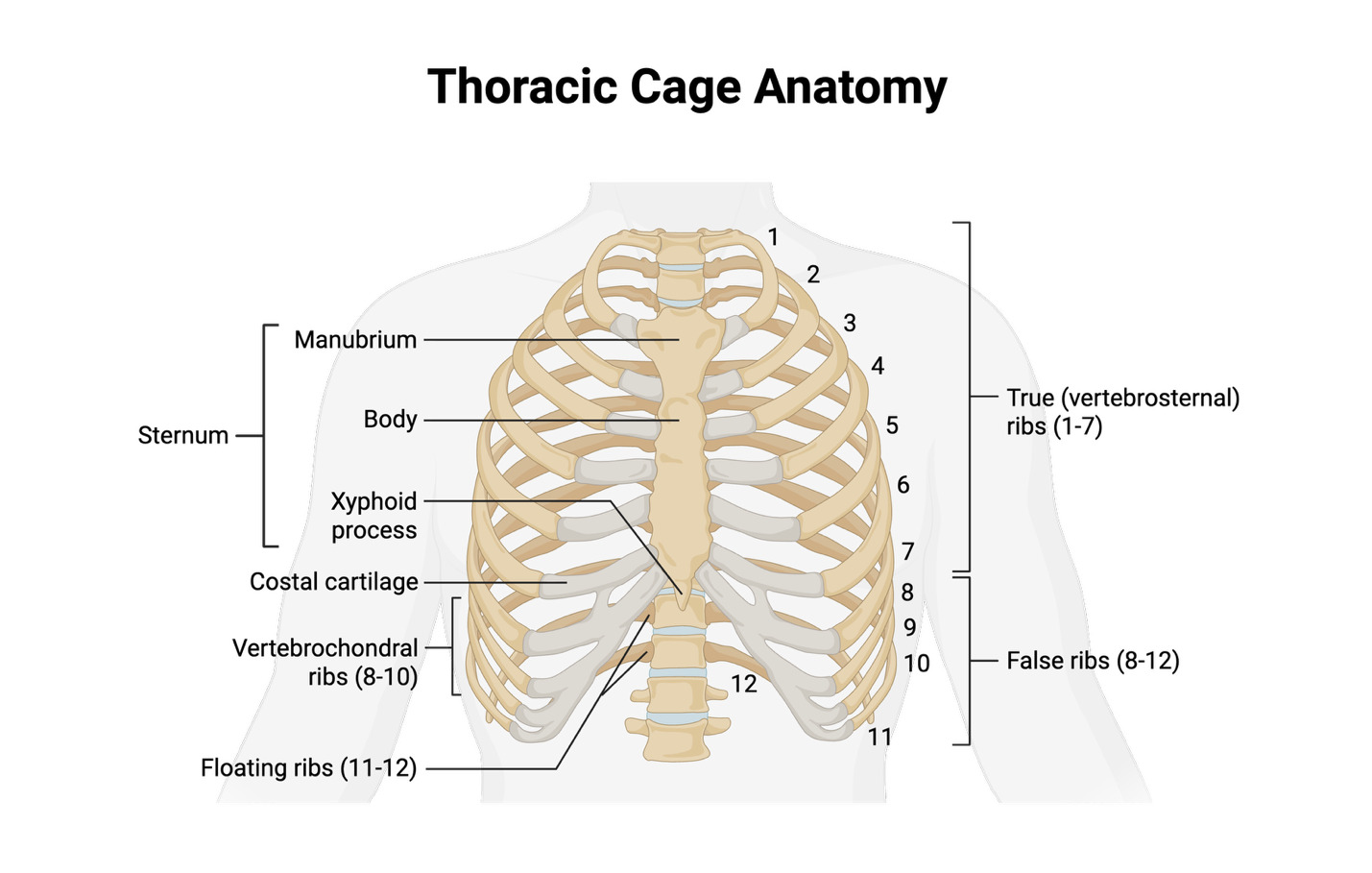
A rib fracture is an injury that occurs when one or more bones in the rib cage breaks or cracks. Rib fractures typically occur when a significant force is directed onto the ribs to cause them to break. Rib fractures can either be traumatic or atraumatic which means that they could either be caused by trauma such as blunt force to the ribs or have a non-trauma related cause such as a severe cough or repetitive stress from athletic activities. Studies have estimated that the incidence of a rib fracture in the ED to be between 9% and 38%,1 demonstrating that they are relatively common, especially in older populations. Rib fractures can occur as either a single or multiple fractures, or as a flail segment where three or more consecutive ribs are fractured in two or more areas.2 A flail segment is a destabilized segment of the chest wall and is typically caused by significant trauma to the chest. There are 12 pairs of ribs in the thoracic region, with rib numbers eight through ten being connected to the cartilage of the sternum and being more vulnerable [Figure 1]. The ribs protect the underlying organs and structures, and as such, fractures can also lead to accompanying injuries. Rib fractures can be associated with notable health complications, such as tears in the arteries and lungs.3
_https___biorender.com_f8fq32l.png)
Every year, an estimated 248,000 people visit the emergency department due to broken ribs in the United States.4 The most common causes of a rib fracture are motor vehicle accidents, incidents involving pedestrian and motor vehicle collisions, falls, and crush injuries.4 Among younger populations, rib fractures are caused due to high-energy traumatic events. In vehicle crashes, impact with the steering wheel or side doors can cause injury to the ribs. In older populations, these fractures often result from falls.5 The elderly are more likely to suffer rib fractures due to their impaired bone strength which is caused by low bone density or other debilitating bone conditions such as osteoporosis.6 Patients will likely report painful thoracic trauma and decreased inspiratory ability due to pain. Physical examination may unveil chest wall bruising, vital sign abnormalities as well as notable respiratory distress. The mainstay of treatment is analgesia, which in this case is achieved with an erector spinae block to provide regional anesthesia.
Case Presentation
A 60-year-old female with no past medical history presented to the emergency department (ED) as a trauma alert after being ejected from her bicycle and landing on her right shoulder. She was wearing a helmet. The patient reported extreme chest, back, and right shoulder pain, and had a depressed level of consciousness with a Glasgow Coma Scale (GCS) of 12 upon arrival. Furthermore, several abrasions were found all on the right side of her body. The patient had neither pain with internal or external rotation of the hip or using her elbow. She did not report any headache, numbness or other complaints. She denied any alcohol or drug use. No obvious deformities were noted. Her vital signs included a temperature of 36.6 degrees Celsius, pulse of 71 beats per minute, blood pressure of 110/61 mmHg, and a respiratory rate of 17 breaths per minute. She had an oxygen saturation of 92% when vital signs were first documented. Laboratory analysis was unremarkable. She was resuscitated per Advanced Trauma Life Support (ATLS) protocol.
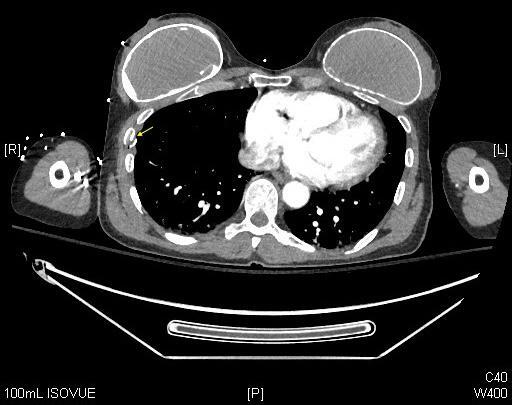
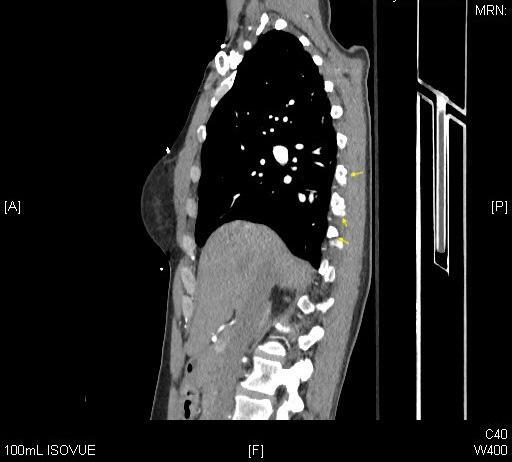
The CT scans of the abdomen and pelvis found no solid organ or hollow viscus injury. Spine CTs were negative for fracture or subluxation of the cervical, thoracic, or lumbar spine. Noncontrast brain CT was also negative for acute pathology. However, CT scans of the chest found right posterolateral third, fourth, fifth, sixth, seventh, eighth rib fractures [Figures 2,3]. A clavicle fracture was also found.
.jpg)
.jpg)
An erector spinae plane (ESP) block was performed on the patient to provide analgesia. This procedure was ultrasound guided and performed at bedside using strict aseptic technique aimed to give regional anesthesia for the right-sided posterior lateral rib fractures to the patient. The patient was positioned prone, and was kept on cardiac and pulmonary monitoring throughout the procedure.
A high-frequency linear probe was placed longitudinally in the parasagittal orientation approximately 3 cm lateral to the transverse process of the spine at T5. A 22-gauge, 100-millimeter (mm) nerve block needle was utilized. Ultrasound guidance with an in-plane approach of the needle was also maintained throughout the procedure. Twenty milliliters (ml) of normal saline was first injected to hydrodissect the fascial plan and ensure placement in the correct place before injecting the 20 ml of 0.25% bupivacaine, followed by additional saline to increase the spread of coverage. The anesthetic was spread in the cranial caudal directions, which allowed for coverage of multiple dermatomes, areas of the skin that rely on nerve connections to the spine, of the back and chest. Fortunately, the patient did not experience any complications from the ESP block, including inadequate pain control, pneumothorax, anesthetic toxicity, infection, or allergic reaction. Analgesia was achieved within minutes. A splint was provided for the clavicle fracture. The patient’s Glasgow Coma Scale quickly improved to 15. The patient was admitted to the trauma service for observation. She was discharged home the next day, and given clinic follow up.
Discussion
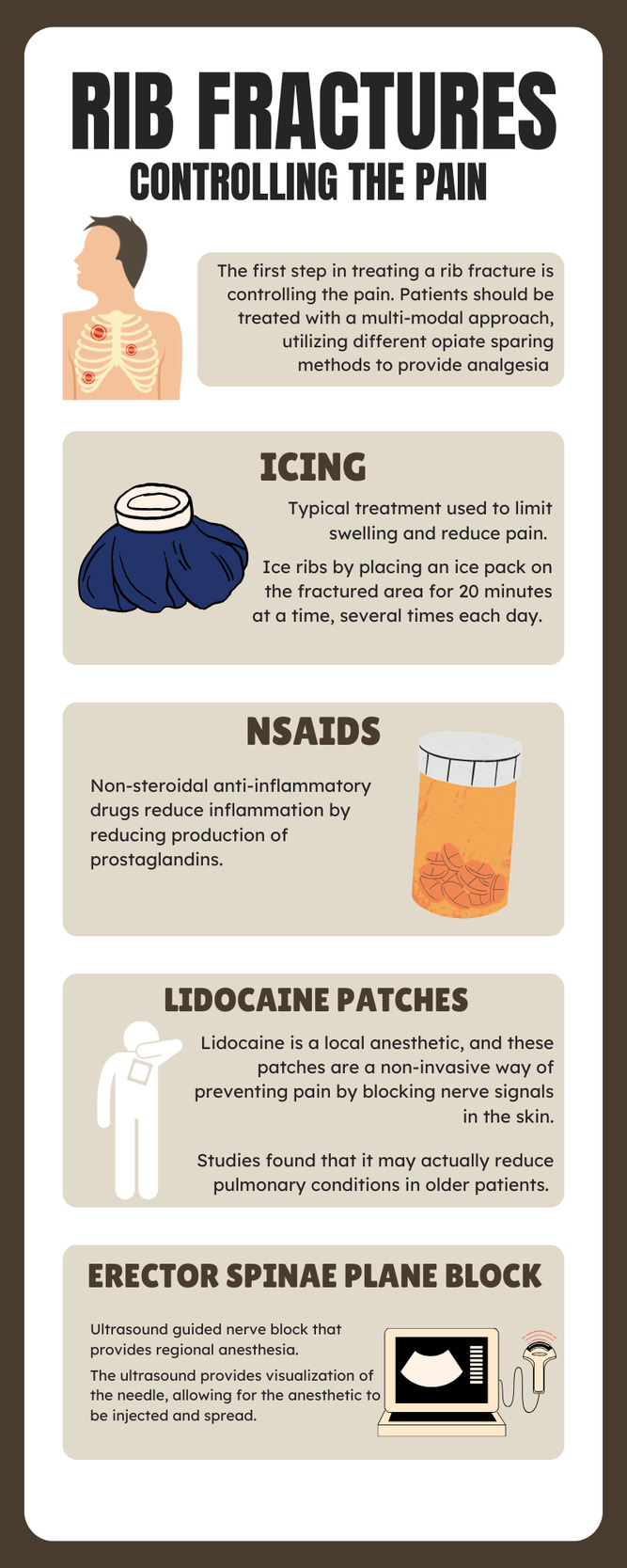
Rib fractures are a common result of high trauma to the chest, and the first step in treating a fractured rib is by controlling the pain.7 This case illustrates the varied approaches that can be taken when both diagnosing and treating a rib fracture. When the patient arrived at the ED, it was seen that the patient had abrasions on the right side of their body and was experiencing chest pain. Furthermore, a CT scan of the chest was performed in the case to identify the broken ribs. CT scans are one of the most common radiological techniques used and have been set as the gold standard.8
Analgesia was achieved in the emergency department with an ESP block, which blocks the dorsal and ventral rami of the thoracic and abdominal spinal nerves by injecting local anesthetic into the paraspinal fascial plane between the tip of the transverse process of the thoracic or lumbar vertebra and the anterior fascia of the erector spinae muscles.9 This avoided the need for opiate analgesia. Opiates can be very sedating, and can cause hypotension, oftentimes provided inadequate analgesia.
Ultrasound guided nerve blocks (UGNB) are becoming more common in the emergency department, as more ED physicians are trained in ultrasonography. A 2025 scoping review identified 238 articles encompassing 9055 individual UGNBs, including 34 randomized controlled trials. The ESP block made up 18 % of the blocks, with a rapid increase over the past 5 years.10
The patient also received other analgesic modalities, including intravenous ketorolac (a non-steroidal anti-inflammatory drug), ice, and a lidocaine patch [Figure 4]. Lidocaine patches have the advantage of lesser systemic absorption, and a lower incidence of pulmonary complications in the elderly.11,12
Conclusion
Rib fractures are associated with significant morbidity and mortality, especially in older adults. Regional anesthesia is an important adjunct in the management of multiple rib fractures. Regional anesthesia, in this case the erector spinae plane block, confers excellent analgesia without the potential adverse effects of opiates, such as sedation and hypotension. Multi-modal analgesia excluding opiates remains the favored approach for pain control when feasible.